

















Probox MushPro S Grow Tent - Garden Highpro
Cultivation Material
€95.00Price
To access our site, you must confirm that you are at least 18 years old.



Imagine the brain as a snow-covered mountain. Every recurring thought, every automatic reaction, and every mental habit is a sled that travels the same path over and over again. Over time, those paths become deep grooves: efficient and fast… but increasingly difficult to leave behind.
This image captures well what happens in many states of psychological rigidity. Chronic stress, anxiety, depression, or even everyday routine reinforce repetitive thinking patterns. Not because they are the best, but because they are the most travelled. The brain, like any biological system, tends to optimize what it already knows.
For decades, it was assumed that this rigidity was, to a large extent, irreversible in adulthood. Today we know it doesn't have to be. The brain retains a remarkable capacity to change, adapt, and reorganize itself. We call this property neuroplasticity.
In recent years, psychedelic mushrooms (particularly species of the genus Psilocybe) have re-emerged in scientific research as possible catalysts of this plasticity. Not only because of the altered states of consciousness they produce, but because of something deeper and more lasting: their ability to induce structural and functional changes in the brain that persist long beyond the acute experience.
This article explores what neuroplasticity really means, how psilocybin acts on the brain, what the current scientific evidence says, and what its implications, limitations, and risks are.
Neuroplasticity is the ability of the nervous system to reorganize itself at different levels: molecular, cellular, structural, and functional. It involves both the creation of new connections and the elimination of those that are no longer adaptive — a natural ‘pruning’ process called synaptic pruning that allows the brain not only to grow, but to refine itself.
For a long time, it was thought that this capacity decreased dramatically after childhood, an idea inherited from early models of brain development. Today we know that the adult brain remains plastic, although that plasticity tends to be more “regulated” and less spontaneously available.
To understand how psychedelics interact with these processes, we need to distinguish several relevant types of plasticity:
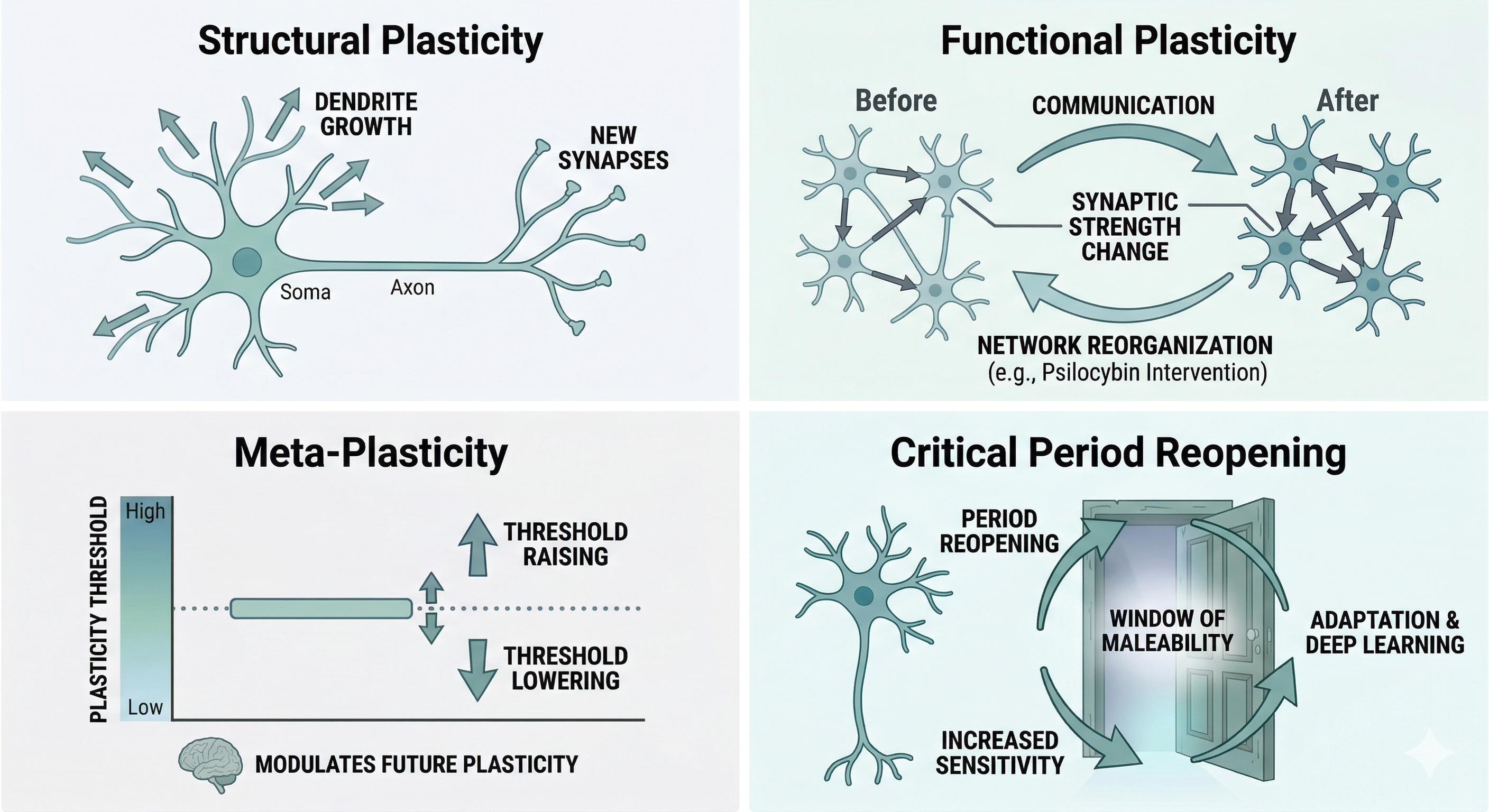
These different types of plasticity provide the conceptual framework for understanding how substances such as psilocybin can induce significant brain changes even in adults.
Psychedelic mushrooms, especially species of the genus Psilocybe, naturally produce psilocybin. It is important to note that psilocybin is, strictly speaking, a prodrug: a substance that is not significantly active on its own, but which the body metabolizes (primarily in the liver) to convert it into psilocin, the molecule that actually crosses the blood-brain barrier and produces effects in the brain.
Unlike many other secondary metabolites produced by fungi and plants, psilocybin shows a remarkable affinity for the human serotonergic system, particularly for certain receptors involved in processes such as perception, cognition, and emotional regulation.
Although they are related, current research suggests that the latter cannot be explained solely by the former. This distinction is crucial, as it suggests that the true therapeutic power of psilocybin may reside not only in the intensity of the subjective experience, but in the biological «window of opportunity» that opens at the cellular level. Understanding the substance as a structural modulator allows us to separate the phenomenon of hallucination from the process of neural repair and rewiring that we will analyze below.
A third element, just as determinant as dose or molecular mechanism, is what researchers call set and setting: the set refers to the participant's internal state — their emotional disposition, expectations, and personal history — while the setting refers to the physical, social, and relational environment in which the experience takes place. In clinical trials, both are carefully controlled through prior preparation, professional support, and subsequent integration sessions. This variable is far from incidental: studies show that the same compound, administered in different contexts, can produce radically different experiences, and that the quality of set and setting partly predicts the magnitude and direction of therapeutic change.
In recent years, a key term has emerged to describe substances like psilocybin: psychoplastogens. The concept, proposed in the context of modern research by teams such as that of David E. Olson, refers to compounds capable of promoting neuroplasticity rapidly and powerfully, beyond their subjective effects.
Before examining the molecular mechanisms, it is worth highlighting a distinction that is often overlooked in popular science coverage of this topic: there is no single “mode of use” for psilocybin, and different administration contexts produce very different biological and therapeutic profiles. In clinical and research settings, two main approaches are distinguished:
It was traditionally thought that activating the 5-HT2A receptors located on the surface of the neuron was sufficient to trigger psychedelic effects. However, recent research has revealed a crucial neurobiological nuance: location.
Unlike endogenous serotonin, which has difficulty crossing the cell membrane due to its polarity, psilocin (and other psychedelics) can cross this lipid barrier and access the interior of the cell. Once inside, it binds to a pool of 5-HT2A receptors located in intracellular organelles, such as the Golgi apparatus.
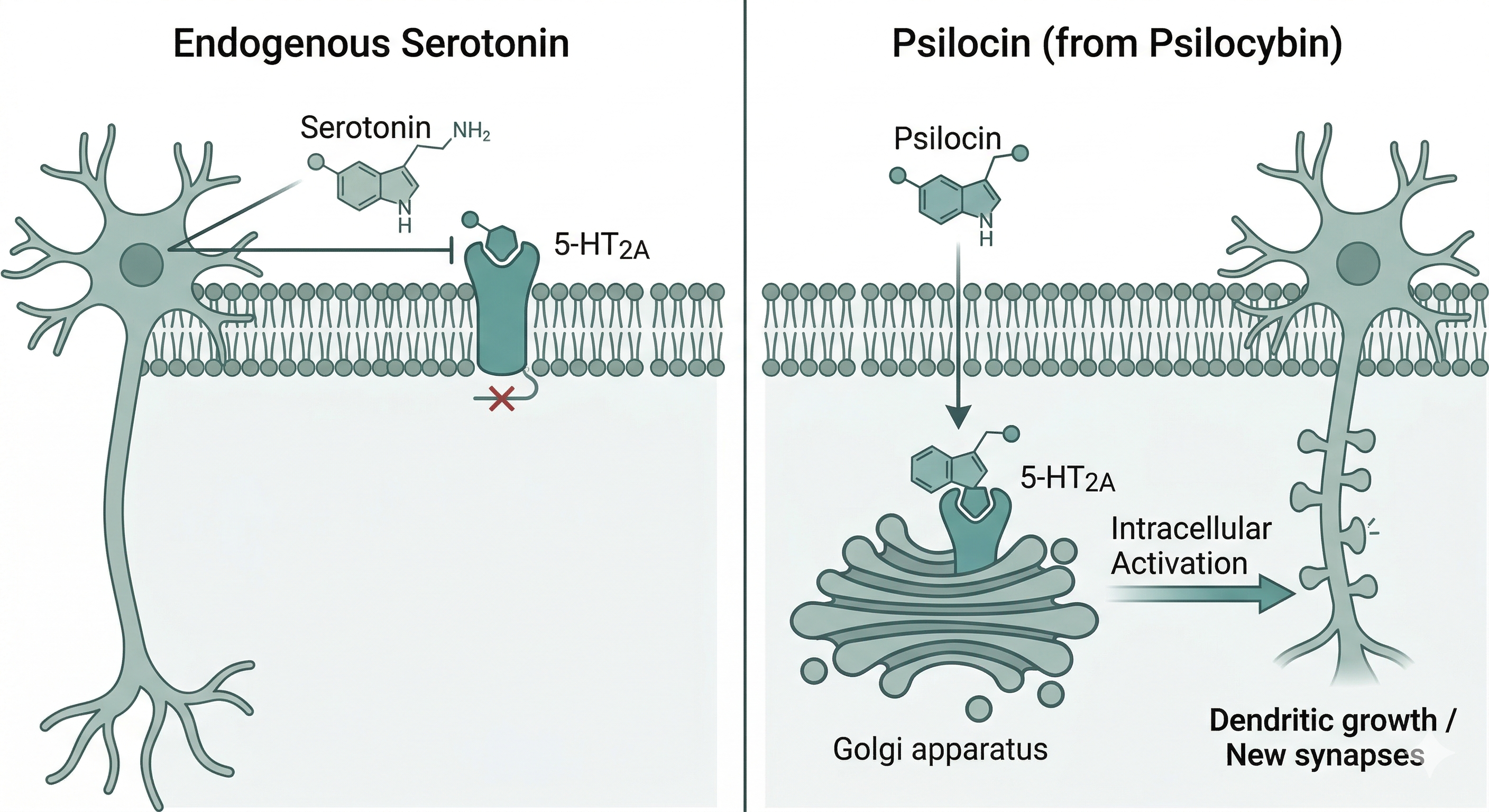
Current evidence suggests that it is precisely this intracellular activation that consistently triggers the growth of dendrites and the formation of new spines. This would explain why, even though we constantly have serotonin in the brain, it does not provoke the deep structural changes or the rapid plasticity states we observe with psychedelics.
One of the key players in this process is BDNF (Brain-Derived Neurotrophic Factor), a protein fundamental to neuronal growth, survival, and differentiation. Psilocybin is associated with an increase in the expression and release of BDNF, which facilitates the activation of its TrkB receptor and contributes to the consolidation of new synaptic connections.
Some studies suggest that certain plastic effects can occur in a partially independent manner from the 5-HT2A receptor, pointing to mechanisms more complex than initially assumed.
These molecular changes potentially translate into a more flexible brain capable of reorganizing its networks, underpinning improvements in learning, adaptation, and emotional regulation.
This effect is further amplified by a mechanism we will address later: the simultaneous reduction of the DMN's ruminative activity, whose chronic hyperactivity acts as an active suppressor of BDNF expression through the stress axis.
Although psilocybin is eliminated from the body within a matter of hours, the changes it induces can persist for weeks or even months. This apparent paradox is explained by the fact that the substance does not act solely as a transient stimulus, but as a trigger for biological processes that continue to unfold once the acute phase has ended.
One of the mechanisms involved is the activation of gene expression programs associated with synaptic plasticity. Psilocybin induces the expression of immediate-response genes and other genes involved in neuronal growth, synapse stabilization, and circuit reorganization. These molecular changes can consolidate over time through the synthesis of new proteins and the structural modification of existing connections.
Moreover, the formation of new dendritic spines and the strengthening of certain synapses are not fleeting processes. Once established, these modifications can integrate in a relatively stable manner into neural networks, especially when accompanied by changes in the individual's experience, behavior, or environment.
At the functional level, psilocybin is also associated with a transient reorganization of brain connectivity dynamics. During this period, the brain can explore less rigid and more flexible configurations. In some cases, certain of these configurations persist after the experience, giving rise to more adaptive processing patterns.
These findings suggest that the duration of the effects does not depend on the continued presence of the substance, but on psilocybin's capacity to initiate a cascade of molecular, structural, and functional changes that, under certain conditions, can consolidate over the medium and long term.
Preclinical studies have been fundamental in characterizing how psilocybin induces plastic changes at the cellular and structural level. In cell cultures, brief exposures to psilocybin or analogous compounds produce significant increases in dendritic complexity and synaptic density within 24 to 72 hours. It is particularly noteworthy that short-duration stimuli can generate effects comparable to those observed after prolonged treatments.
In animal models, a single administration is associated with an increase in dendritic spine density in key regions such as the medial prefrontal cortex and the hippocampus. These changes can persist for several weeks, and even more than a month. Furthermore, in chronic stress models, psilocybin reverses stress-induced dendritic atrophy and is associated with improvements in indicators of adaptive behavior.
These findings provide solid mechanistic support that justifies the exploration of psilocybin in clinical studies in humans.
To understand the psychological and therapeutic effects of psilocybin, it is essential to discuss the Default Mode Network (DMN), a set of highly interconnected brain regions that act as an organizing axis of internal experience.
The DMN is particularly active when we are not engaged in a specific task oriented toward the outside world. It is associated with the narrative of the self, autobiographical memory, mental planning, and the constant evaluation of oneself. When its activity is excessive or rigid, it is linked to patterns of rumination, self-criticism, and repetitive thinking.
Psilocybin significantly reduces the coherence and functional dominance of this network. It is as if the brain's “manager” — the system that centralizes, prioritizes, and gives continuity to experience — temporarily steps back. This decline in hierarchical control correlates with the decrease in synchronized activity within the DMN and is what many people subjectively describe as ego dissolution.
When this control relaxes, global connectivity between brain networks increases. Regions that normally operate in a more segregated fashion begin to exchange information more directly. This less restrictive connectivity pattern has been associated with phenomena such as synesthesia, deep cognitive reframing, and the emergence of unusual perspectives.
This increase in global connectivity translates into what neuroscience describes as an increase in brain entropy: the brain operates in a broader state space, with less predictable and more variable activation patterns. Far from being a sign of pathological disorganization, this elevated entropy reflects a brain temporarily freed from its most rigid perceptual and cognitive routines — more similar, in terms of network dynamics, to the brain of a child exploring the world than to that of an adult solving the familiar.
From a neuroplasticity standpoint, a brain that is less hierarchical and less constrained by dominant internal models is a more malleable brain. This window of flexibility is key to understanding why certain psilocybin-induced experiences can facilitate lasting psychological change.
Before examining the specific studies, it is worth framing the current state of the field. Clinical research on psilocybin has advanced considerably over the past decade, but continues to operate with relatively small samples, heterogeneous protocols, and a structural limitation that is difficult to resolve: true double-blinding is virtually impossible when participants can clearly perceive whether they received the active substance. This does not invalidate the findings — the consistency of effects across different groups, institutions, and methodologies is itself a strong signal — but it does require reading the results with the precision that any science in progress deserves.
The most influential trials come from the group of Robin Carhart-Harris, initiated at Imperial College London and subsequently continued at the University of California San Francisco. Their studies with patients who had not responded to multiple lines of conventional pharmacological treatment documented significant reductions in depressive symptomatology after one or two psilocybin sessions integrated into a psychotherapeutic support protocol.
In functional neuroimaging, this work revealed a persistent reduction in DMN activity weeks after the intervention, correlated with clinical improvement.
The same group subsequently led a trial with a different population: patients with moderate-to-severe depression without treatment-resistance criteria. The trial published in The New England Journal of Medicine in 2021 compared psilocybin with the antidepressant escitalopram and showed comparable results on the primary symptom scale — though the primary endpoint did not reach statistical significance, in part due to sample size — and superior results for the psilocybin group on several secondary measures of emotional wellbeing. Escitalopram showed a faster response in the first weeks, suggesting that the two interventions have distinct and potentially complementary temporal profiles.
The group of Roland Griffiths at Johns Hopkins University has produced some of the most carefully designed trials in the field. In a randomized controlled study with oncology patients carrying a potentially life-threatening diagnosis, a single high dose of psilocybin produced clinically significant reductions in both anxiety and depression, which remained stable in follow-ups conducted at six months. In approximately 80% of participants, the beneficial effects were still perceptible in long-term assessments — a level of persistence unusual in psychopharmacology. The authors also observed that the intensity of the mystical experience during the session correlated with the magnitude of the subsequent therapeutic benefit, fueling debate about the relevance of the experiential component in the mechanism of action.
Research has yielded notable preliminary results. The Johns Hopkins group published a pilot study on tobacco dependence in which two or three psilocybin sessions combined with cognitive-behavioral therapy produced six-month abstinence rates above 60%, well above the historical benchmarks of first-line treatments. For alcohol use disorder, a controlled trial from New York University reported sustained and significant reductions in consumption compared to active placebo. Both lines of research are still in their early stages in terms of sample size and require replication, but the magnitude of the observed effects justifies the growing interest.
Functional and structural neuroimaging techniques show changes in connectivity between prefrontal and subcortical regions weeks after a single administration. These modifications affect circuits involved in emotional regulation, decision-making, and stress response. Variations in cortical thickness have also been described in areas related to cognitive control and emotional integration.
At the psychological level, sustained improvements have been documented in cognitive flexibility, emotional empathy, and subjective wellbeing. These changes are not accompanied by a deterioration of basic cognitive functions, such as working memory or attention, which reinforces the safety profile observed in controlled studies.
In controlled therapeutic settings, particularly for treatment-resistant depression or anxiety, beneficial effects can be maintained for months and even up to a year after one or two sessions, always integrated within a framework of psychological support.
| Condition | Institution | Key Finding |
|---|---|---|
| Treatment-Resistant Depression | Imperial College / UCSF | Rapid improvement; superior to common medications for long-term wellbeing. |
| Terminal Anxiety | Johns Hopkins University | 80% success rate with sustained clinical improvement after 6 months. |
| Tobacco Addiction | Johns Hopkins University | 60% abstinence at 6 months (doubles conventional efficacy). |
| Alcohol Use | NYU | Significant reduction in heavy drinking days versus active placebo. |
Psilocybin induces real brain changes. That means the risks are also real. The clearest example is HPPD (Hallucinogen Persisting Perception Disorder): visual distortions that reappear weeks or months after the experience. It is the most direct demonstration that more plasticity does not automatically equate to “better” plasticity: in certain individuals, processing circuits consolidate in unwanted ways.
For this window of malleability to be therapeutic rather than destabilizing, prior medical screening and context are non-negotiable. Without a safety framework and subsequent integration, the brain may reinforce maladaptive patterns rather than breaking them. The following are the systematic medical and pharmacological exclusion criteria used in clinical research:
Precision in screening is what separates a transformative experience from an unnecessary risk. For a detailed technical analysis of each interaction and safety protocol, you can consult our complete guide to risks and contraindications of psilocybin.
After the psychedelic experience, the brain remains in a state of elevated plasticity for days or weeks. Returning to our initial metaphor: fresh snow covers the old grooves. But the snow does not decide on its own which new paths are formed. If there are no changes in the environment, habits, or therapeutic support, the weight of repetition will reopen exactly the same grooves as before. And that has consequences in both directions.
This is why integration is fundamental. The evidence indicates that psilocybin is not a panacea, but a modulator: a signal that the brain interprets to build — or eliminate — real connections at the molecular, structural, and functional level.
This process can persist for months after a single session, offering genuine therapeutic implications for depression, anxiety, and addiction. However, the effects depend on context, and the field remains a science in progress. In a territory where biology and subjective experience overlap, precision is not a detail: it is the starting point.
Related posts

Therapeutic applications of psilocybin
Published :
2025-07-31 14:25:24

Psilocybin: what it is, how it works and what effects it has
Published :
2025-07-24 12:21:12

Myths about psilocybin that science has debunked
Published :
2025-12-10 20:34:04